
Diphtheria
Background
Diphtheria can involve almost any mucous membrane. For clinical purposes, it is convenient to classify diphtheria into a number of manifestations, depending on the site of disease: respiratory diphtheria, Anterior nasal diphtheria, pharyngeal and tonsillar diphtheria, laryngeal diphtheria and cutaneous diphtheria.
Taiwan Centers for Disease Control (Taiwan CDC) had listed diphtheria as the second category of notifiable infectious disease, and all people are the monitoring subjects. The medical institutes have to inform cases within 24 hours in accordance with the provision. Whenever the diphtheria is isolated from the pseudomembranous lesions in the throat, larynx and nasal mucosa from suspected cases, the notification should be done as soon as possible. The isolates have to send to Taiwan CDC for further identification to determine the infection cases.
The case-fatality rate for diphtheria has changed very little during the last 50 years. The overall case-fatality rate for diphtheria is 5%-10%, with higher death rates (up to 20%) among persons younger than 5 and older than 40 years of age. Before there was treatment for diphtheria, the disease was fatal in up to half of cases.
Epidemiology
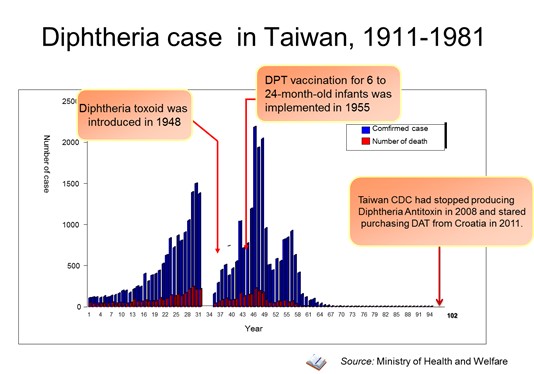
Diphtheria once was a major cause of illness and death among children who were under 15 of years. Taiwan has recorded 2,186 cases of diphtheria in 1957, and then has dropped to 4 cases till 1980. There has been no confirmed case after 1981. However, the disease continues to play a role globally. The cases of diphtheria were reported worldwide to the World Health Organization (WHO), but many more cases likely go unreported.
Diphtheria toxoid was introduced to Taiwan in 1948. DPT vaccination for 6 to 24 month-old infants was implemented in 1955. The incidence was 126 cases per 10,000 people in 1957, and dropped to 0.02 cases per 10,000 people by 1980. There was no more confirmed case after 1981.
Diphtheria can involve almost any mucous membrane. For clinical purposes, it is convenient to classify diphtheria into a number of manifestations, depending on the site of disease: respiratory diphtheria, Anterior nasal diphtheria, pharyngeal and tonsillar diphtheria, laryngeal diphtheria and cutaneous diphtheria.
Taiwan Centers for Disease Control (Taiwan CDC) had listed diphtheria as the second category of notifiable infectious disease, and all people are the monitoring subjects. The medical institutes have to inform cases within 24 hours in accordance with the provision. Whenever the diphtheria is isolated from the pseudomembranous lesions in the throat, larynx and nasal mucosa from suspected cases, the notification should be done as soon as possible. The isolates have to send to Taiwan CDC for further identification to determine the infection cases.
The case-fatality rate for diphtheria has changed very little during the last 50 years. The overall case-fatality rate for diphtheria is 5%-10%, with higher death rates (up to 20%) among persons younger than 5 and older than 40 years of age. Before there was treatment for diphtheria, the disease was fatal in up to half of cases.
Epidemiology
Diphtheria once was a major cause of illness and death among children who were under 15 of years. Taiwan has recorded 2,186 cases of diphtheria in 1957, and then has dropped to 4 cases till 1980. There has been no confirmed case after 1981. However, the disease continues to play a role globally. The cases of diphtheria were reported worldwide to the World Health Organization (WHO), but many more cases likely go unreported.
Diphtheria toxoid was introduced to Taiwan in 1948. DPT vaccination for 6 to 24 month-old infants was implemented in 1955. The incidence was 126 cases per 10,000 people in 1957, and dropped to 0.02 cases per 10,000 people by 1980. There was no more confirmed case after 1981.
Diphtheria case in Taiwan
Diphtheria Surveillance in Taiwan
Taiwan National Infectious Disease Statistics System
Diphtheria
Prevention and Control
- Diphtheria Antitoxin
- After the provisional clinical diagnosis is made and appropriate cultures are obtained, persons with suspected diphtheria should be given diphtheria Antitoxin and antibiotics in adequate dosage and placed in isolation. Respiratory support and airway maintenance should also be administered as needed. In Taiwan, diphtheria antitoxin can be obtained from CDC on request.
- Diphtheria Vaccination
- Vaccination is the best way to prevent diphtheria. Diphtheria toxoid has been introduced to Taiwan since 1948, Diphtheria, tetanus, pertussis (DTP) vaccine was provided in 1954, and 5 in 1 vaccine (Diphtheria, tetanus, pertussis, Hib and polio, DTaP-Hib-IPV) has been introduced in March of 2010. The Diphtheria immunization efficacy will be around 97% after receiving 4 doses of DTaP-Hib-IPV, and the validity is 10 years.
- Preventive Measures
- For diphtheria cases (especially the laryngeal diphtheria and cutaneous diphtheria.), bacterial cultures should be negative for two times. If there was no culture, the isolation and antibiotic should be given for 14 days.
- For close contacts, especially household contacts, the nasal and throat specimen should be taken and health management need to be implemented for 7 days. One diphtheria toxoid booster for unvaccinated persons should be given. Contacts who have immunity deficiency should also receive antibiotics-Oral erythromycin or intramuscular penicillin. People engaged in food processing or the staff of childcare should stop work until no suspicion of carrier.
Images

Attached Files
PublishTime 2014/11/24
:::

 Government Entry Point」(open in new window)")
Taiwan Centers for Disease Control
TEL:886-2-2395-9825
Copyright © 2025 Taiwan Centers for Disease Control. All rights reserved.